The SARS-CoV-2 Omicron variant and its subvariants have posed significant challenges to global public health since their emergence in late 2021. This comprehensive review examines the epidemiological trends, clinical impacts, and public health challenges associated with Omicron subvariants, with a focus on high-density populations such as Bangladesh. The review highlights the evolution of Omicron subvariants, including BA.1, BA.2, BA.4/BA.5, XBB, BQ.1, EG.5, and JN.1, emphasizing their increased transmissibility, immune evasion, and varying severity. Despite lower intrinsic severity compared to Delta, Omicron's rapid spread has strained healthcare systems, particularly in regions with limited resources. In Bangladesh, Omicron subvariants such as XFG, XFC, and NB.1.8.1 have driven recent surges, with test positivity rates peaking at 20% in June 2025. The review underscores the persistent threat of these subvariants, especially among vulnerable populations like the elderly, and the critical need for enhanced genomic surveillance, vaccination campaigns, and adaptive public health strategies. Some of the key challenges include vaccine hesitancy, healthcare infrastructure limitations, and socioeconomic barriers. The findings advocate for robust global cooperation, updated vaccines, and targeted interventions to mitigate the ongoing impact of Omicron subvariants in high-risk settings.
After the World Health Organization’s (WHO) declaration of the SARS-CoV-2 pandemic in March 2020, more than 775 million COVID-19 cases and over 7 million deaths had been reported globally as of June 2024 [1]. The WHO regularly listed updates on variants of concern, which are COVID variants with an increased rate of transmission, virulence, or resistance against mitigations, like vaccines. The predominant strains during the COVID-19 pandemic have been the Alpha, Delta, and Omicron varieties. The Delta variant of SARS-CoV-2 is known to cause more severe illness compared to earlier or later variants. The original Wuhan-Hu-1 strain was less transmissible than alpha, which was discovered in the UK towards the end of 2020. In April 2021, delta, which was even more severe and transmissible, appeared in India. When Omicron was discovered in South Africa in December 2021, it brought about significant mutations in spike proteins, which allowed it to spread quickly. Omicron is 30% more likely to result in death and 40% more likely to result in hospitalization than Delta, which indicates that it typically causes less serious illness [2, 3]. It's difficult to pinpoint a single "global average" case fatality rate (CFR) for each variant of concern, as it is time- and population-dependent, e.g., early waves had higher CFR due to lack of treatments/vaccines. Beyond this, the approximate CFR of the Delta variant was higher than the ancestral (~1.5–2.5%) due to increased severity, and vaccines reduced fatalities. Omicron shows (a) much lower CFR (~0.1–0.7%) due to immunity (vaccines/infections) and reduced intrinsic severity [4].
In 2022, the Omicron variant's successive sub-lineages (BA.1, BA.2, BA.4, and BA.5) were in circulation. Subsequent strains of the Omicron sublineages known as XBB emerged between January and December 2023; these strains have not been attributed to any significant increases in incidence. In August 2023, a new strain of Omicron, known as BA.2.86, was identified. Its genome differed greatly from that of the most common XBB strains. A related strain known as JN.1 had begun to predominate and was linked to a slight increase in activity, becoming the dominant variant over December 2023 and January 2024, although there had been no significant emergence of BA.2.86 by early 2024 [5, 6]. Subvariants of the JN.1 variants have since become more common; in mid-2024, KP.1/KP.2 (referred to as "FLiRT" variants) and KP.3 (referred to as "FLuQE" variants) were linked to an increase in COVID-19 activity. The prevalence of two variants rose during the end of 2024 and the start of 2025: XEC, a recombinant of KP3.3 and KS.1.1, and KP.3.1.1, a further sublineage of the previously circulating KP.3 variant [7, 8]. Additionally, KP.3, LB.1, LP.8.1, and NB.1.8.1 are the variants being monitored, and JN.1 is a variant of interest (VOI) as defined by the World Health Organization [7, 9].
As of May 11, 2025, the global SARS-CoV-2 infection has increased with an 11% test-positive rate in 73 reporting countries. This rate is an alarming rise from just 2% in February 2025 and is comparable to what was observed in July 2024 (12%) [10]. Southeast Asia, the Western Pacific, and the Eastern Mediterranean are the main sources of the current surge. However, while some regions, such as the Caribbean and Andean subregions, have noticed upward trends, the African, European, and Americas regions are reporting lower positivity rates (2–3%). In North America and Europe, the situation is stable, and there are no indications that the virus is spreading more widely [10, 11]. A new variant under observation, NB.1.8.1, is increasing and currently makes up 10.7% of examined cases, while the previously dominant LP.8.1 is decreasing. This evidence suggests that the virus is still evolving. Even though the number of cases is comparable to that of 2024, SARS-CoV-2 still lacks an unusual seasonal pattern [11]. This demonstrates the continuing necessity of robust worldwide surveillance systems.
Since the emergence of the Omicron variant of SARS-CoV-2, multiple subvariants have been detected in Bangladesh over time. However, it is challenging to provide exact statistics on the total number of confirmed cases for each Omicron subvariant in the country. One study reported that BA.1 and BA.2 were the predominant subvariants circulating during January and February 2022. Additionally, Omicron BA.4 and BA.5 were identified between June and July 2022, followed by the detection of the XBB variant from July to October 2022 [12]. Another study documented 81 cases of Omicron BA.1, 290 cases of BA.2, 63 cases of BA.5, and 32 cases of XBB reported in Bangladesh between December 2021 and October 2022 [13]. More recently, in April 2025, two newly emerged Omicron subvariants—XFG and XFC, both descendants of the JN.1 lineage were detected in Bangladesh [14].
Despite relatively lower severity in clinical outcomes compared to Delta, rapid transmissibility of various types of subvariants of Omicron has placed continued pressure on the healthcare system, surveillance infrastructure, and public health preparedness of some South Asian countries like Bangladesh, India where population density is very high. Understanding the epidemiological trends, clinical implications, and public health challenges posed by Omicron variants is crucial for guiding policy decisions in a high-density populated country like Bangladesh. This review aims to provide a comprehensive overview of the emergence and progression of Omicron subvariants, their epidemiological patterns, clinical features, diagnostic and vaccine efficacy, and the effectiveness of public health responses by accumulating available data.
2. OVERVIEW OF OMICRON SUBVARIANTS
2.1. Comparative Prevalence, Severity, Mortality, and Vaccine Efficacy of Omicron Subvariants
Five years into the pandemic, there are now over 30 known variants of the original COVID-19 strain. Variant classification is a keyway to inform countries when new SARS-CoV-2 variants appear that could affect the spread or severity of COVID-19. Therefore, to track and study these variants, WHO categorizes them into three groups named as follows [15].
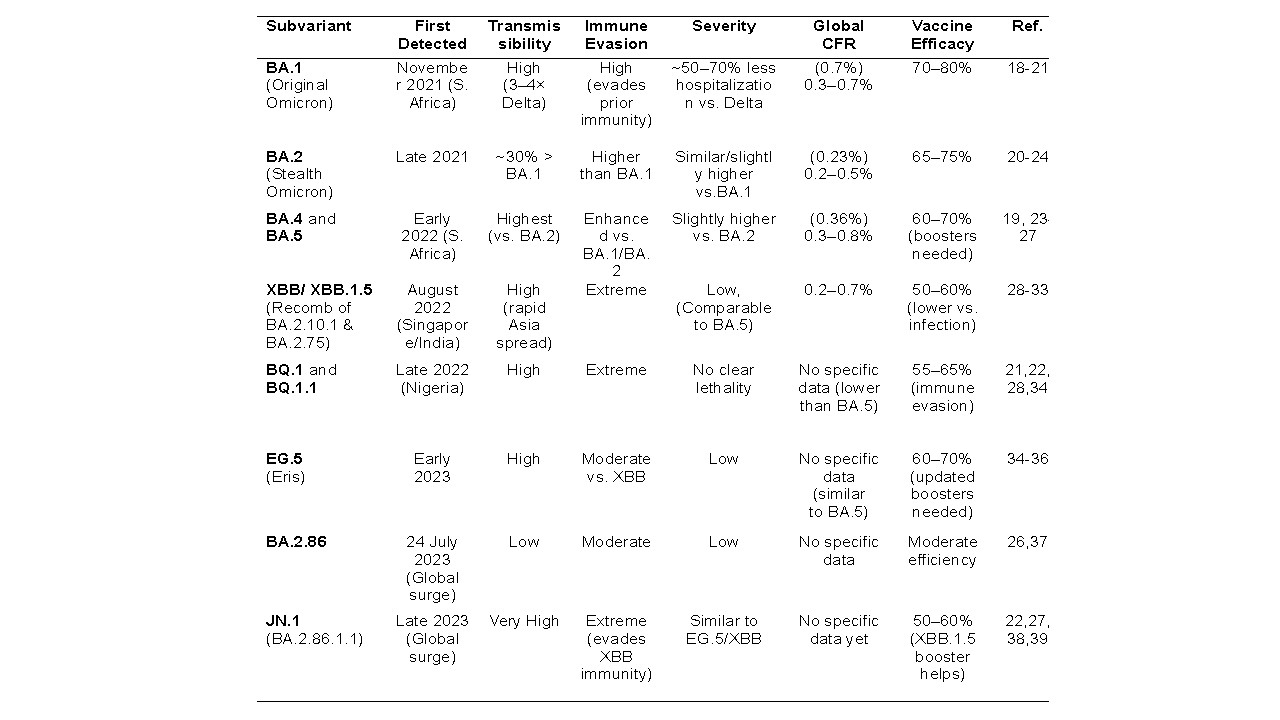
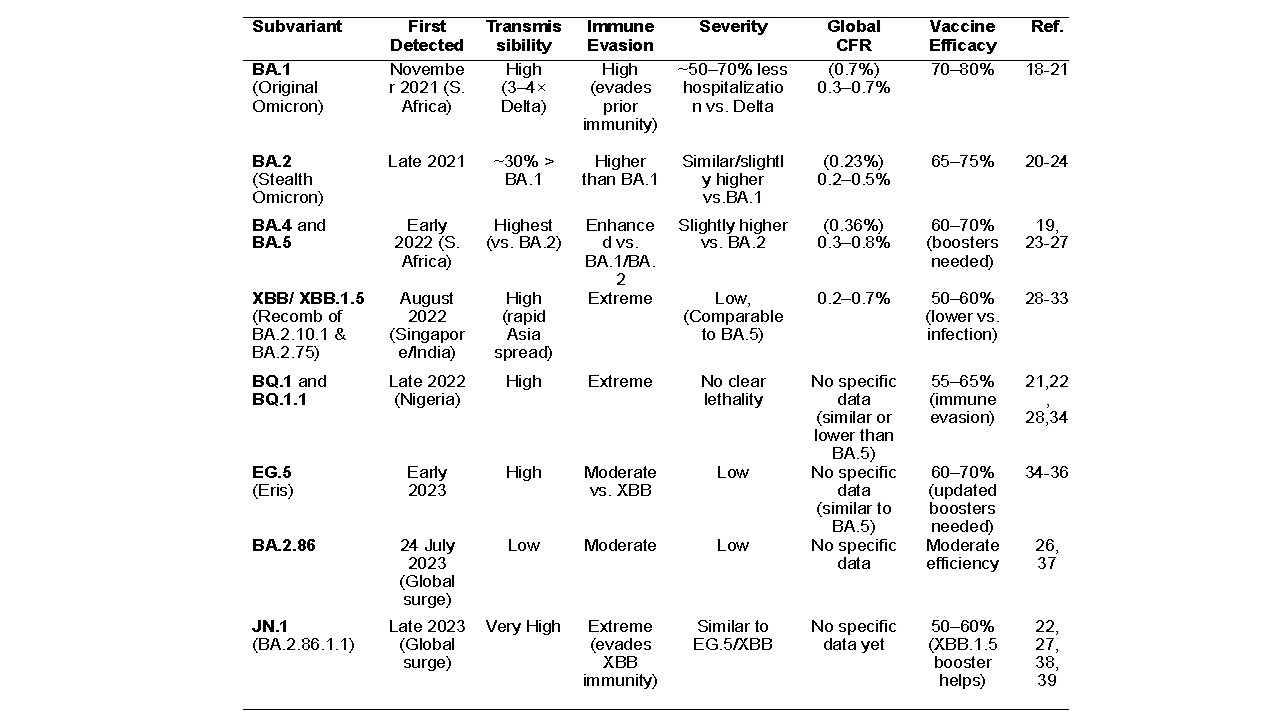
(i) Variants of Concern (VOC)-A VOC is a SARS-CoV-2 variant that shows evidence of increased transmissibility, more severe disease, and has a measurable impact on public health. As of 3 March 2023, BA.2, BA.4, and BA.5 are the SARS-CoV-2 variants of concern (VOC) [16]. (ii) Variants of Interest (VOI) -Emerging SARS-CoV-2 variants that have genetic changes known to affect virus characteristics such as transmissibility, disease severity, or immune escape, and have been identified to cause significant community transmission. At present, WHO recognizes JN.1 as a VOI. (iii) Variants Under Monitoring (VUM)-Very new type of evolving variants that scientists are keeping an eye on but are not yet considered a major threat. For example, in early 2025, a new VUM named XEC emerged as the most prevalent Omicron subvariant worldwide, with the symptoms being similar to those of the previous COVID-19 Omicron strain [16]. As shown in Table 1, this section will focus on selected Omicron subvariants, while details on other emerging VOI and VUM will be covered in the next part. Table 1 provides a comparative overview of key Omicron subvariants of SARS-CoV-2, detailing their transmissibility, immune evasion, severity, global case fatality rate (CFR), and vaccine efficacy against severe disease. The data is drawn from multiple studies, as referenced below, offering insights into the evolving characteristics of these subvariants. The overview study shows that the basic and effective reproduction numbers of the Omicron variant are, respectively, 8.2 and 3.6 on average, which means in terms of basic reproduction number and effective reproduction number, Omicron variants were 2.5 and 3.8 times more transmissible than the Delta variant, respectively [17].
BA.1 (Original Omicron): First detected in South Africa in November 2021, BA.1 exhibited high transmissibility (3–4 times that of Delta) and significant immune evasion, bypassing prior immunity. It was 50–70% less likely to cause hospitalization compared to Delta, with a global CFR of 0.3–0.7%. Vaccine efficacy against severe disease ranged from 70–80% [18-21]. Studies highlight its reduced pathogenicity compared to Delta [18, 20].
Table 1. Summary of basic information of different types of SAR-COV-2 Omicron subvariants.
BA.2 (Stealth Omicron): Emerging in late 2021, BA.2 was approximately 30% more transmissible than BA.1 and showed higher immune evasion. Its severity was similar to or slightly higher than BA.1, with a CFR of 0.2–0.5%. Vaccine efficacy against severe disease was slightly lower at 65–75% [4, 20, 21] with a slight increase in hospitalization rates compared to BA.1 [20, 22].
BA.4 and BA.5: Detected in early 2022 in South Africa, these subvariants were more transmissible than BA.2 and exhibited enhanced immune evasion. Severity was slightly higher than BA.2, with a CFR of 0.3–0.8%. Vaccine efficacy dropped to 60–70%, with boosters necessary for optimal protection [21, 23-27]. Studies confirm increased immune escape and clinical severity compared to earlier Omicron lineages [25, 26].
XBB/XBB.1.5: A recombinant of BA.2.10.1 and BA.2.75, first identified in August 2022 in Singapore and India. XBB/XBB.1.5 spread rapidly in Asia due to high transmissibility and extreme immune evasion. Its severity was low, comparable to BA.5, with a CFR of 0.2–0.7%. Vaccine efficacy against severe disease was reduced to 50–60%, particularly against infection [28-33].
BQ.1 and BQ.1.1: Emerging in late 2022 in Nigeria, these subvariants showed high transmissibility and extreme immune evasion. Severity data is limited, but lethality appears similar to or lower than BA.5. The CFR for Omicron subvariants BQ.1 and BQ.1.1 is not explicitly documented in the provided references or recent studies. Vaccine efficacy was estimated at 55–65%, impacted by immune evasion [21, 22, 34]. Their clinical outcomes are similar to BA.5 [28].
EG.5 (Eris): A subvariant of Omicron’s XBB lineage, was first identified in February 2023 and classified as a VOI by WHO on August 8, 2023, due to its high transmissibility and moderate immune evasion linked to the F456L spike mutation. Despite its rapid spread, there is no evidence of increased severity or mortality. Although no specific case fatality rate (CFR) is documented, it seems too similar to BA.5. Vaccine effectiveness is estimated at 60–70%, with updated boosters recommended. WHO and CDC consider EG.5 a low public health risk [34–36].
BA.2.86: The omicron subvariant BA.2.86 is a descendent lineage of BA.2, with the earliest sample collected on 24 July 2023. There is no evidence that BA.2.86 has additional public health risks like severity, transmissibility, etc., relative to the other currently circulating Omicron descendent lineages [37]. BA.2.86 has over 30 spike mutations compared to XBB.1.5, including changes in key antigenic sites (e.g., K356T, V445H, N450D, G446S), which help it escape antibody recognition [26, 37]. Ongoing monitoring is needed as the variant evolves.
JN1 (BA.2.86.1.1): JN.1, a descendant of BA.2.86, emerged in late 2023 as a VOI and is characterized by a single additional spike protein mutation (L455S) compared to BA.2.86, enhancing its immune evasion and transmissibility. JN.1 exhibited very high transmissibility and extreme immune evasion even against XBB-induced immunity with no specific CFR data available [24, 38, 39]. Severity was comparable to EG.5/XBB, with 50–60% vaccine efficacy, though XBB.1.5-based boosters provided some protection [21, 22, 27, 39]. Despite its rapid global spread, there is no evidence that JN.1 causes more severe disease or higher mortality than other Omicron subvariants [39].
2.2.CFR of Omicron Subvariants
The case fatality rate (CFR) is a measure used in epidemiology to assess the severity of a disease. It represents the proportion of deaths among confirmed cases of the disease within a specific time period. The CFR can vary depending on factors like population demographics, vaccination status, and healthcare access. However, General Omicron CFRs range from 0.16% (Taiwan, 2022–2023) to 0.70% (global meta-analysis), with BA.5 sublineages at 0.36%. BQ.1 and BQ.1.1, as BA.5 derivatives, likely have similar or lower CFRs due to Omicron’s reduced severity compared to Delta, even though their immune evasion may increase case burdens. Meta-analysis on CFR for Omicron was 0.70%, with sublineage rates for BA.1 (0.98%), BA.2 (0.23%), and BA.5 (0.36%). No specific mention of BQ.1 or BQ.1.1 [4].
2.3. Distinct Clinical Features of Different Omicron Subvariants
Based on available data, comparative clinical and epidemiological characteristics of the main Omicron subvariants have been summarized in Table 2. Due to increased immune evasion, most of the subvariants have changed symptomatology, duration of illness, and reinfection risks over time, as stated below.
Symptom Shift: A sore throat, fatigue, and nasal congestion were common in early Omicron subvariants (BA.1, BA.2); however, there was a reduced fever and a less frequent loss of taste and smell in later variants (XBB, JN.1). Gastrointestinal symptoms were more prevalent in JN.1 and BA.2 [40-45, 48, 50, 51].
Immune Evasion: Progressive mutations that effectively evade prior hybrid immunity, such as F456L in EG.5 and spike changes in JN.1, increased the risk of reinfection. These mutations also peaked with XBB.1.5. Therefore, Evusheld and other monoclonal antibodies lost their effectiveness against XBB, BQ.1, and JN.1 [45, 47, 50, 54].
Clinical Severity: Most subvariants caused milder disease than the Delta variant, though elderly and unvaccinated individuals remained at higher risk of severe outcomes, particularly with BQ.1.1 and JN.1 [48, 54, 55].
Prolonged Illness: Omicron variants may have a lower risk of long COVID compared to Delta because of persistent symptoms (fatigue, cough). Still, some new variants (XBB, JN.1) are associated with longer symptom duration (7–14 days) and raise concerns about long COVID [47, 54, 55].
Age-Specific Effects: Children were more likely to suffer from mild illnesses (such as croup with BA.1), and older people were more likely to require hospitalization, particularly if they were not properly vaccinated [44-51].
Reinfection Trends: Due to immune escape, the first significant waves of reinfection were driven by XBB and BA.4/BA.5. Even in people who have already contracted XBB variants, JN.1 is causing reinfections [44-48, 51, 54].
Table 2. Comparative clinical features of Omicron subvariants.
3. THE GLOBAL RISING TRENDS OF OMICRON SUBVARIANTS
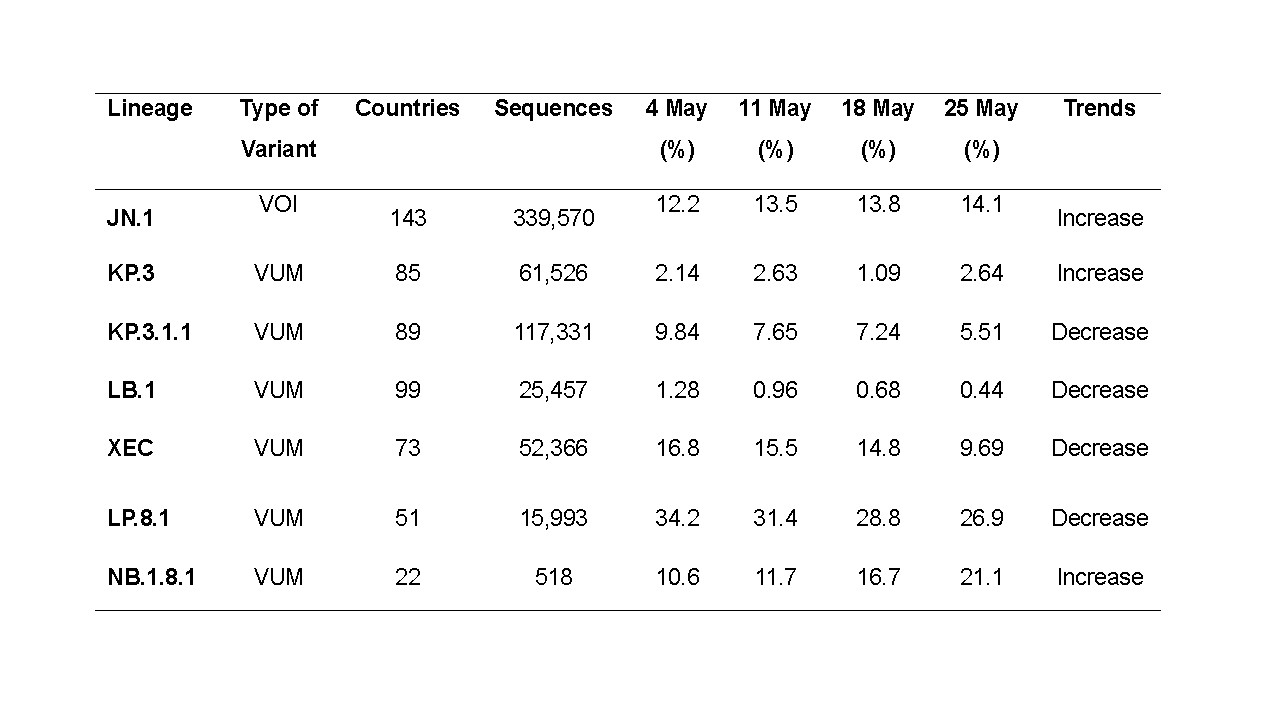
Since early 2025, global SARS-CoV-2 variant trends have slightly shifted. Since mid-February 2025, global SARS-CoV-2 activity has been on the rise, with sentinel site data showing a test positivity rate of 11%—the highest since July 2024 [56]. This increase is most noticeable in the Eastern Mediterranean, Southeast Asia, and Western Pacific regions. In May 206,279 new cases were reported, a significant jump from 27,134 cases in April across 93 countries. Particularly, this surge was largely driven by a single WHO region i.e. South-East Asia, where thereported number of new cases rose from 71 in April to 182,010 in May, accompanied by an increase in test positivity from 1.3% to 5.8%. [56]. Especially in the region of Southeast Asian countries, including Thailand, Singapore, and Hong Kong, and including India and Bangladesh. In early 2025, the dominant Omicron subvariants worldwide were classified by the WHO into two categories: (i) Variants of Interest (VOI) and (ii) Variants Under Monitoring (VUM). A brief overview of each is provided in the following section, and their emerging trends have been summarized briefly in Table 3data derived from the COVID-19 dashboard.[56, 57].
Variants of Interest (VOI): As of May 2025, only JN.1 subvariant is listed as a VOI by WHO, a descendant of BA.2.86, highly contagious, causing milder symptoms, and able to partially evade immunity. Brief characteristics of JN.1 have been discussed in Tables 1and 2 [57].
Variants Under Monitoring (VUM): As of May 2025, according to WHO's recent classification, newly evolved subvariants such as KP.3, KP.3.1.1, JN.1.18, LB.1, LP.8.1, and NB.1.8.1 are in the VUM category because of their mutations, which could impact transmission and immune evasion. LP.8.1 dominates U.S. cases (73%), followed by XFC (10%) and XEC (4%) as of May 2025. Some of their major characteristics are stated as follows.
XEC: In early 2025, a new COVID-19 variant called XEC has become the dominant global strain. Created by combining two Omicron subvariants (KS.1.1 and KP.3.3), XEC was first detected in Germany in June 2024 and has since spread rapidly [58].
NB.1.8.1 and LF.7: A new COVID-19 variant, identified in January 2025 is NB.1.8.1, also called Nimbus, has been identified in several Asian countries, including India, Hong Kong, Singapore, and Thailand. This variant, a descendant of the Omicron subvariant JN.1 [59]. The WHO has designated NB.1.8.1 as a VUM due to its increasing prevalence and potential public health implications. [59, 60]. Like earlier Omicron strains, NB.1.8.1 carries spike protein mutations that enhance spread with low disease severity or significantly evade immunity. NB.1.8.1 is particularly notable for its rapid spread, with commonly reported symptoms including sore throat, fatigue, mild cough, fever, muscle aches, and congestion.
XFG: First identified in Canada, is being detected increasingly in India 163 cases were reported in June, marking a moderate surge in transmissibility. Like other Omicron descendants, XFG mostly causes mild illness. Data on severity remain limited pending further observation [61].
Table 3. Rising trends of SARS-CoV-2 Omicron subvariants up to May 2025.
4. TRENDS OF OMICRON SUBVARIANTS IN BANGLADESH: A 24-MONTH OVERVIEW (JUNE 2023 – JUNE 2025)
As part of the ongoing surveillance of SARS-CoV-2 dynamics in high-density regions, Bangladesh presents a compelling case study of fluctuating epidemiological patterns shaped by variant emergence, public health interventions, and population immunity. In Bangladesh between December 2021 and October 2022, Omicron subvariants BA.1, BA.2, BA.5, and XBB were reported [13]. Very recently, in April 2025, two newly emerged Omicron subvariants—XFG and XFC, both descendants of the JN.1 lineage were detected in Bangladesh [14]. As of 08 June 2025, according to a report by the Directorate General of Health Services Bangladesh, new coronavirus subvariants—particularly Omicron subtypes BA 2.86, XFG, XFC, and JN.1—are on the rise with previously identified XBB. Moreover, the daily positivity rate of Covid-19 has surged to 20 percent in June 2025, up from just 9.51 percent in May, whereas from January to August 2024, this rate was around 1.5% only [63].
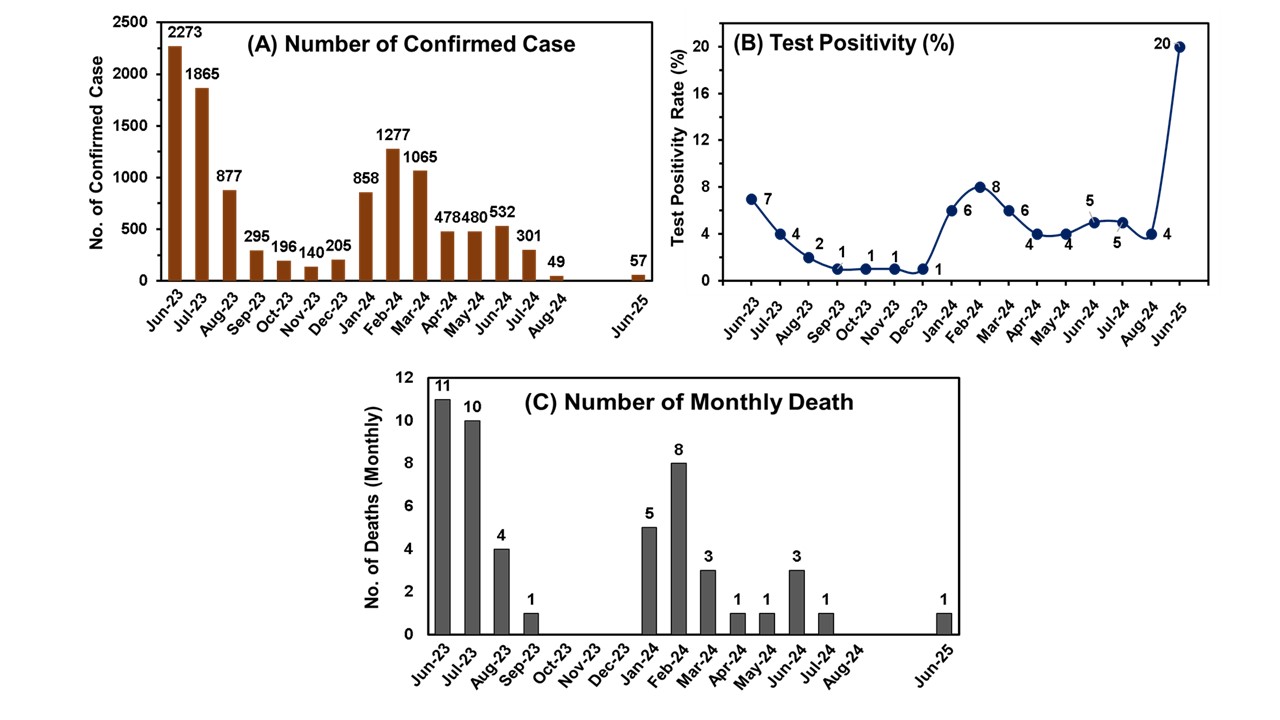
Therefore, potential public health risks in Bangladesh can be assessed by analyzing the epidemiological trends of COVID-19 over the past 24 months (from June 12, 2023, to June 8, 2025), based on data provided by the Directorate General of Health Services (DGHS) [63]. To understand the possible risk, Figure 1 summarizes the total number of confirmed cases, test positivity rates, and reported deaths during this period. Among the 10,948 confirmed cases, more than half occurred in individuals aged 25–34 years, followed by those aged 35–44 years. Male patients accounted for approximately 40% more cases than females. Notably, around 60% of the reported deaths occurred in individuals aged over 60 years, highlighting increased vulnerability among the elderly population. More detailed discussions are provided below.
4.1. Confirmed Case Patterns: An early wave of high transmission was observed in mid-2023, with the highest monthly incidence recorded in June 2023 (~23,00 confirmed cases), followed closely by July (~19,00 cases). This surge was followed by a sharp decline, stabilizing below 200 cases/month by November 2023. From January to March 2024, confirmed cases slightly increased, with an average of about 1000. Then, from April to August 2024, Bangladesh experienced a prolonged period of low-level community transmission, averaging 50–500 confirmed cases per month. However, starting from April, there was a dramatic spike in the first week of June 2025 [63, 64].
4.2. Test Positivity Rate: The test positivity rate—an important metric for viral circulation—mirrored case trends. It declined from a peak of ~7% in June 2023 to ~1% by the end of 2023. Throughout most of 2024, the rate hovered at a stable low of ~4–8%, indicating sustained control of the virus. Alarmingly, in May and June 2025, the positivity rate surged sharply, reaching approximately 20% in June—the highest during the two-year review period—signaling a significant outbreak and suggesting potential emergence of a new, more transmissible Omicron subvariant [62, 63].
4.3. Mortality Trends: COVID-19-related deaths showed a continuous decline across the 24 months. From ~10 deaths/month in mid-2023, mortality dropped significantly to fewer than 1 death/month by the end of that year. During most of 2024 and early 2025, the monthly death toll remained in the single digits, 1-3 deaths/month (except in January and February 2024, with 5 and 8 deaths, respectively). However, in spite of the increasing positivity rate, the monthly death rate did not increase yet. It is very necessary to continue this controlling situation to avoid further outbreaks [63].
However, in 2025, newly identified highly transmissible Omicron subvariants like XFG, XFC, and NB.1.8.1 may pose a threat to the COVID-19 outbreak in any country with a large population density, such as Bangladesh.
Figure 1. Summary statistics of SARS-CoV-2 in Bangladesh over the past 24 months (from 12 June 2023 to 8 June 2025), including total confirmed cases, positivity rate, and number of deaths [63]. *Gaps indicate periods with unavailable data or no reported cases.
5. PUBLIC HEALTH CHALLENGES AND PREVENTIVE STRATEGIES
The emergence of the Omicron variant of SARS-CoV-2 has posed significant challenges to global public health, including in overpopulated, low- and middle-income countries (LMICs) like Bangladesh. Characterized by high transmissibility and immune evasion, Omicron led to a surge in cases, although with reduced severity compared to previous variants. This review examines the prevalence, epidemiology, transmissibility, clinical burden, mortality, and previous records of Omicron in Bangladesh, contextualizing it within global trends. Therefore, future challenges followed by preventive measures have been discussed below.
5.1. Challenges to Control Outbreak
High Transmissibility in Dense Populations: Omicron subvariants, such as XBB, XFG, and XFC, are highly transmissible. In Bangladesh, crowded urban slums (e.g., Dhaka, Chattogram) and public transport systems may facilitate rapid viral spread. This section outlines key challenges and notable limitations.
Limited Healthcare Infrastructure: Bangladesh’s healthcare system is fragile, including inadequate testing (5,000 tests per million for about 170 million people), and hospital capacity hinders timely case detection and management. A new Omicron variant could strain resources, especially in rural areas with poor access to testing and treatment.
Vaccine Hesitancy and Low Coverage: Low vaccination rates may be caused by the use of different vaccine types and inconsistent distribution of recommended booster doses, limited public awareness, and a lack of enough willingness to receive the vaccine. In addition, waning immunity can increase the risk of serious consequences, especially for older and immunocompromised people.
Socioeconomic Barriers: Socioeconomic constraints such as poverty, low education, and occupational vulnerabilities (e.g., day laborers, garment workers), inconsistent mask-wearing, and hygiene practices limit adherence to preventive measures.
Behavioral Factor: The general population's tendency to overlook or inadequately follow health instructions is a key contributor to the rapid spread of COVID-19 in overpopulated countries.
5.2. Challenges of Dengue and COVID-19 Coinfection in Bangladesh
A major public health concern in Bangladesh is the co-occurrence of dengue fever and COVID-19, leading to diagnosis, treatment, and the distribution of medical resources becoming more difficult. Without appropriate testing, differential diagnosis is challenging since both conditions exhibit overlapping clinical symptoms, such as fever, headache, and muscle pain [65]. Seasonal dengue epidemics and the ongoing COVID-19 threat have coexisted in Bangladesh, resulting in confirmed coinfection cases. Coinfected people often experience worse clinical outcomes, such as longer hospital stays and increased risks of comorbidities like thrombocytopenia and respiratory failure [66]. Considering both conditions required distinct but related medical treatments, the burden on the healthcare system grows even more [67]. Preventive measures, including vector control for dengue and vaccination/social distancing for COVID-19, must be integrated to mitigate dual outbreaks [68].
5.3. Preventive Strategies
Enhanced Genomic Surveillance and Early Detection: Establish a national genomic surveillance program and partner with international databases (e.g., GISAID) to track mutations. Implement wastewater surveillance, as demonstrated in South Africa, to detect variants in communities before clinical cases surge. As an immediate response, the authorities can implement the following effective measures.
Reinforced Vaccination Campaigns: Accelerate vaccination, prioritizing boosters tailored to Omicron subvariants (e.g., XBB.1.5, JN.1). Address hesitancy through community-based education campaigns in local languages, targeting low-literacy groups. Mobile vaccination units should reach slums and rural areas, ensuring equitable access. Make a collaboration with NGOs, garment industry leaders, social media, and religious leaders to vaccinate workers.
Proper Allocation of Improved Healthcare Resources: Allocate COVID patient health service-related latest equipment and facilities to upgrade health services, especially for rural, vulnerable, crowded urban slum people, and establish temporary treatment centers in high-density areas. Make a collaboration with international organizations for resource support.
Public Health Measures: Implement appropriate initiatives to encourage adherence to WHO-recommended practices, such as mask-wearing, hand hygiene using sanitizers, and ensuring adequate ventilation in indoor spaces.
Community Engagement: Tailor risk communication to low-education groups using mobile apps, SMS, TV, radio, social media, community influencers, and local leaders. Launch door-to-door education campaigns, focusing on preventive behaviors and vaccine benefits.
6. CONCLUSIONS
The continuous evolution of SARS-CoV-2 Omicron subvariants, characterized by heightened transmissibility and immune evasion, underscores the persistent challenges in managing the COVID-19 pandemic, particularly in high-density, resource-limited regions like Bangladesh. While these subvariants generally exhibit reduced severity compared to earlier variants, their rapid spread and ability to evade immunity have led to recurrent surges, straining healthcare systems and disproportionately affecting vulnerable populations such as the elderly and unvaccinated. The recent dominance of subvariants like XFG, XFC, and NB.1.8.1 highlights the need for sustained genomic surveillance, adaptive public health strategies, and equitable access to updated vaccines. Addressing vaccine hesitancy, strengthening healthcare infrastructure, and fostering global collaboration are critical to mitigating the ongoing impact of Omicron subvariants. Moving forward, a proactive, data-driven approach—combining robust surveillance, targeted vaccination campaigns, and community engagement—will be essential to curbing transmission and safeguarding public health in the face of an ever-evolving virus.
ACKNOWLEDGEMENT
We gratefully acknowledge the contributions of researchers, students, and public health organizations worldwide whose efforts in tracking, analyzing, and reporting on SARS-CoV-2 variants have been invaluable. Special thanks to the Directorate General of Health Services (DGHS), Bangladesh, for providing essential data and insights. Finally, we extend our gratitude to all frontline responders whose dedication continues to mitigate the impact of COVID-19 globally.
FUNDING SOURCES
This research received no external funding.
CONFLICT OF INTEREST
Author has no conflict of interest
ETHICS STATEMENT
This article is a review of previously published literature and does not involve any new studies with human participants or animals performed by the author. Therefore, ethical approval was not required. All sources have been appropriately cited to acknowledge the original authors.
Khan S, Yahiro T, Kimitsuki K, Hashimoto T, Matsuura K, et al. Exploring the replication and pathogenic characteristics of alpha, delta, and omicron variants of SARS-CoV-2. Int J Mol Sci. 2024;25(23):12641.
Nyberg T, Ferguson NM, Nash SG, et al. Comparative analysis of the risks of hospitalization and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: a cohort study. Lancet. 2022;399(10332):1303-1312.
Xia Q, Yang Y, Wang F, Huang Z, Qiu W, et al. Case fatality rates of COVID-19 during epidemic periods of variants of concern: a meta-analysis by continents. Int J Infect Dis. 2024; 141:106950.
Saberiyan M, Karimi E, Khademi Z, Movahhed P, Safi A, et al. SARS-CoV-2: phenotype, genotype, and characterization of different variants. Cell Mol Biol Lett. 2022; 27:50.
Lim ZJ, Subramaniam A, Ponnapa Reddy M, Blecher G, Kadam U, Afroz A, Billah B, Ashwin S, Kubicki M, Bilotta F, Curtis JR, Rubulotta F. Case Fatality Rates for Patients with COVID-19 Requiring Invasive Mechanical Ventilation. A Meta-analysis. Am J Respir Crit Care Med. 2021;203(1):54-66. doi:10.1164/rccm.202006-2405OC
Lytton SD, Ghosh AK, Bulbul RH, Nafisa T, Mamunur R, et al. The severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) omicron sub-variants in Bangladesh cause mild COVID-19 and associate with similar antibody responses irrespective of natural infection or vaccination history. Heliyon. 2024;10(10): e31011.
Jubair M, Begum MN, Rahman S, Haider SMA, Moon SB, et al. SARS-CoV-2 Omicron variants in Bangladesh: pandemic to endemic. Health Sci Rep. 2023;6(3): e1134.
Kumar S, Karuppanan K, Subramaniam G. Omicron (BA.1) and sub-variants (BA.1.1, BA.2, and BA.3) of SARS-CoV-2 spike infectivity and pathogenicity: a comparative sequence and structural-based computational assessment. J Med Virol. 2022;94(10):4780-4791.
Twohig KA, Nyberg T, Zaidi A, Thelwall S, Sinnathamby MA, Aliabadi S, Seaman SR, Harris RJ, Hope R, Lopez-Bernal J, Gallagher E, Charlett A, De Angelis D, Presanis AM, Dabrera G; COVID-19 Genomics UK (COG-UK) consortium. Hospital admission and emergency care attendance risk for SARS-CoV-2 delta (B.1.617.2) compared with alpha (B.1.1.7) variants of concern: a cohort study. Lancet Infect Dis. 2022;22(1):35-42. doi:10.1016/S1473-3099(21)00475-8
Andrews N, Stowe J, Kirsebom F, et al. COVID-19 vaccine effectiveness against the omicron (B.1.1.529) variant. N Engl J Med. 2022;386(16):1532-1546.
Lewnard JA, Hong VX, Patel MM, et al. Clinical outcomes associated with SARS-CoV-2 omicron (B.1.1.529) variant and BA.1/BA.1.1 or BA.2 subvariant infection in Southern California. Nat Med. 2022;28(9):1933-1943.
He Q, An Y, Zhou X, Xie H, Tao L, et al. Neutralization of EG.5, EG.5.1, BA.2.86, and JN.1 by antisera from dimeric receptor-binding domain subunit vaccines and 41 human monoclonal antibodies. Med. 2024;5(5):401-413.e4.
Strasser ZH, Greifer N, Hadavand A, Murphy SN, Estiri H. Estimates of SARS-CoV-2 Omicron BA.2 Subvariant Severity in New England. JAMA Netw Open. 2022;5(10): e2238354.
Nakakubo S, Kishida N, Okuda K, et al. Associations of COVID-19 symptoms with omicron subvariants BA.2 and BA.5, host status, and clinical outcomes in Japan: a registry-based observational study. Lancet Infect Dis. 2023;23(11):1244-1256.
Moustsen-Helms IR, Bager P, Larsen TG, et al. Relative vaccine protection, disease severity, and symptoms associated with the SARS-CoV-2 omicron subvariant BA.2.86 and descendant JN.1 in Denmark: a nationwide observational study. Lancet Infect Dis. 2024;24(9):964-973.
Lewnard JA, Hong V, Kim JS, et al. Association of SARS-CoV-2 BA.4/BA.5 Omicron lineages with immune escape and clinical outcome. Nat Commun. 2023;14(1):1407.
Wolter N, Jassat W, Walaza S, et al. Clinical severity of SARS-CoV-2 Omicron BA.4 and BA.5 lineages compared to BA.1 and Delta in South Africa. Nat Commun. 2022;13(1):5860.
Qu P, Xu K, Faraone JN, et al. Immune evasion, infectivity, and fusogenicity of SARS-CoV-2 BA.2.86 and FLip variants. Cell. 2024;187(3):585-595.e6.
Ao D, He X, Hong W, Wei X. The rapid rise of SARS-CoV-2 Omicron subvariants with immune evasion properties: XBB.1.5 and BQ.1.1 subvariants. MedComm (2020). 2023;4(2): e239.
Zhang H, Li B, Sun J, et al. Immune evasion after SARS-CoV-2 Omicron BA.5 and XBB.1.9 endemic observed from Guangdong Province, China from 2022 to 2023. Virol J. 2024; 21:298.
Ma KC, Surie D, Lauring AS, et al. Effectiveness of Updated 2023-2024 (Monovalent XBB.1.5) COVID-19 Vaccination Against SARS-CoV-2 Omicron XBB and BA.2.86/JN.1 Lineage Hospitalization and a Comparison of Clinical Severity-IVY Network, 26 Hospitals, October 18, 2023-March 9, 2024. Clin Infect Dis. 2024; ciae405.
Kopel H, Araujo AB, Bogdanov A, et al. Effectiveness of the 2023-2024 Omicron XBB.1.5-containing mRNA COVID-19 Vaccine (mRNA-1273.815) in Preventing COVID-19-related Hospitalizations and Medical Encounters Among Adults in the United States. Open Forum Infect Dis. 2024;11(12): ofae695.
Nguyen JL, Guevara M, Singson JRC, et al. Effectiveness of the BNT162b2 XBB.1.5-adapted vaccine against COVID-19 hospitalization related to the JN.1 variant in Europe: a test-negative case-control study using the id.DRIVE platform. eClinicalMedicine. 2024; 79:102995.
Li H, Yang C, Yin L, et al. Comparative immunogenicity of monovalent and bivalent adenovirus vaccines carrying spikes of early and late SARS-CoV-2 variants. Emerg Microbes Infect. 2024;13(1):2387447.
Centers for Disease Control and Prevention. SARS-CoV-2 B.1.1.529 (Omicron) Variant - United States, December 1-8, 2021. MMWR Morb Mortal Wkly Rep. 2021; 70:1731-1734.
Sievers C, Zacher B, Ullrich A, et al. SARS-CoV-2 Omicron variants BA.1 and BA.2 both show similarly reduced disease severity of COVID-19 compared to Delta, Germany, 2021 to 2022. Euro Surveill. 2022;27(22):2200396.
Møller Kirsebom FC, Andrews N, Stowe J, et al. Effectiveness of the COVID-19 vaccines against hospitalization with Omicron sub-lineages BA.4 and BA.5 in England. Lancet Reg Health Eur. 2023; 23:100537.
Pedersen RM, Bang LL, Tornby DS, et al. Omicron BA.5 Neutralization among Vaccine-Boosted Persons with Prior Omicron BA.1/BA.2 Infections. Emerg Infect Dis. 2022;28(12):2575-2577.
Tan CY, Chiew CJ, Pang D, et al. Protective immunity of SARS-CoV-2 infection and vaccines against medically attended symptomatic omicron BA.4, BA.5, and XBB reinfections in Singapore: a national cohort study. Lancet Infect Dis. 2023;23(7):799-805.
Yue C, Song W, Wang L, et al. ACE2 binding and antibody evasion in enhanced transmissibility of XBB.1.5. Lancet Infect Dis. 2023;23(3):278-280.
Akash S, Islam MR, Dhama K. Emergence BQ.1 and BQ.1.1 as newly identified omicron subvariants: current scenario and future outlook - an update. Ann Med Surg (Lond). 2023;85(4):1329-1330.
Planas D, Bruel T, Staropoli I, et al. Resistance of Omicron subvariants BA.2.75.2, BA.4.6, and BQ.1.1 to neutralizing antibodies. Nat Commun. 2023;14(1):824.
Rajsri KS, Singh M, Rao M. Efficacy of COVID-19 Vaccines against the Omicron Variant of SARS-CoV-2: A Review. Explor Res Hypothesis Med. 2024;9(2):128-137.
Siddiqui AN, Musharaf I, Gulumbe BH. The JN.1 variant of COVID-19: immune evasion, transmissibility, and implications for global health. Ther Adv Infect Dis. 2025; 12:20499361251314763.
Sheten T, Clements ACA, Gray DJ, Adhikary RK, Wangdi K. Clinical features and outcomes of COVID-19 and dengue co-infection: a systematic review. BMC Infect Dis. 2021;21(1):729. doi:10.1186/s12879-021-06409-9
Sharif N, Opu RR, Khan A, Saha T, Masud AI, et al. Clinical epidemiology of dengue and COVID-19 co-infection among the residents in Dhaka, Bangladesh, 2021–2023: a cross-sectional study. Open Forum Infect Dis. 2025;12(2): ofaf039. doi:10.1093/ofid/ofaf039
Rahman MM, Bodrud-Doza M, Shammi M, Islam ARMT, Khan ASM, et al. COVID-19 pandemic, dengue epidemic, and climate change vulnerability in Bangladesh: scenario assessment for strategic management and policy implications. Environ Res. 2021; 192:110303. doi: 10.1016/j.envres.2020.110303
Jal S, Chhotaray S, Pattnaik G, Mishra S, Mohapatra RK, et al. Dengue fever coinfection in COVID-19 era: a public health concern. Health Sci Rep. 2024;7(5): e2089. doi:10.1002/hsr2.2089
 access
access